The reunion of wisdom, care and method in 21st century medicine
Quality of life, functional health and the Medicine of interfaces
Publisher: World Organization of Dermophthalmology (WOD) — Dermophthalmology.com
Prepared by: Scientific Working Group on Dermophthalmology & Functional Interfaces
About this White Paper (Purpose & Scope)
This White Paper:
• Describes a unifying clinical framework (Dermophthalmology) and not a new medical specialty.
• Focuses on chronic functional conditions of high impact on daily life, exemplified by ocular surface diseases.
• Links Ophthalmology with Dermatology, ENT and Allergology in an evidence-based manner, through the concept of functional interfaces (eyelid–tear film–skin–nasal pathway).
• Supports the clinical value of patient-reported outcomes (PROs) and prevention/hygiene as evidence-based interventions.
Intended audience: Ophthalmologists, Dermatologists, ENT, Allergists, General/Family Physicians, health professionals, academic institutions, Public Health organizations.
Table of Contents
1. Abstract
2. Executive Impact Statement
3. Key Messages
4. Acknowledgements & Scientific Recognition
5. Part I — Before Hippocrates: Medicine as Wisdom, Context and Initiation
6. Part II — Asclepius: From Wisdom to Therapeutic Practice
7. Part III — Hippocrates: The Revolution of Method
8. Part IV — What Was Lost After: When the Triad Became a Unit
9. Part V — The Modern Paradigm: When the Patient Has Symptoms but “Has Nothing”
10. Part VI — The Birth of Dermo-Ophthalmology: The Reunion of the Triad in Modern Medicine
11. Part VII — Hygiene & Prevention: When Care Becomes Everyday Medical Practice
12. Part VIII — Changing Attitudes: Quality of Life, Public Health and the Future of Medicine
13. Epilogue
14. References
15. Abbreviations
From Chiron to Hippocrates and Dermo-Ophthalmology
Reconnecting the Forgotten Foundations of Medicine with Quality of Life in Modern Healthcare 21st century global medicine is characterized by unprecedented technological progress, high diagnostic accuracy and impressive therapeutic results in acute and life-threatening diseases. At the same time, however, there is a growing discrepancy between scientific competence and the lived experience of patients, especially in chronic, functional conditions that profoundly affect quality of life without easily fitting into classical nosological patterns. This White Paper argues that this contradiction is not a failure of modern medicine, but the result of a historical transition, during which method — although necessary and life-saving — prevailed over synthesis. Through an analysis of the original triad of medical thought — wisdom and context (Chiron), therapeutic practice and care (Asclepius), systematic method (Hippocrates) — the text highlights how Medicine evolved from a holistic art of living to a primarily method-centric scientific system. Using modern Ophthalmology as an illustrative and globally relevant example, the White Paper examines conditions such as dry eye, blepharitis, allergic rhinoconjunctivitis, and meibomian gland dysfunction — conditions with a high impact on the functionality and daily lives of millions of people. Scientific data from Ophthalmology, Dermatology, Otolaryngology and Allergology document that the eyelids and ocular surface constitute a critical functional interface between skin, tear film and nasal passages, with a direct impact on visual comfort and quality of life (1–5, 9–12, 17–20). Dermo-ophthalmology is presented as a modern, unifying scientific framework that does not question existing specialties, but functionally connects them, restoring the lost framework between symptom, experience and scientific interpretation. With an emphasis on prevention, interface hygiene and patient-reported outcomes, Dermo-ophthalmology responds to the modern needs of a anthropocentric, sustainable and collaborative Medicine (21–22, 29–30). In full alignment with international Public Health frameworks — such as those promoted by the World Health Organization (WHO) — this White Paper recognizes that chronic conditions with low mortality but high impact on functionality are a strategic priority for modern health systems (23–27). It is argued that the reunion of method, care and wisdom is not a return to the past, but a necessary evolutionary step for the future of global Medicine. This text aspires to function as a founding point of reference: not only for the scientific understanding of Dermo-Ophthalmology, but also for a broader repositioning of Medicine around quality of life, prevention and the human experience of health.Executive Impact Statement
Why this White Paper matters. This White Paper highlights a critical gap in modern medicine: the increasing burden of chronic conditions with low mortality but high impact on functionality and quality of life, which often remain under-recognized by traditional diagnostic frameworks (23–27). Using ocular surface disorders as a typical and globally relevant example, the text demonstrates how symptoms often precede objective findings, leading to underdiagnosis, fragmented care, and alienation of patients from the health system (6–8). By introducing Dermo-Ophthalmology as a unifying clinical framework — rather than a new specialty — the White Paper functionally reconnects Ophthalmology, Dermatology, Otolaryngology, and Allergology into a single model of understanding. The proposed approach is aligned with contemporary public health priorities, which emphasize function, patient-reported outcomes, and prevention (23–27, 29–30). Its adoption can reduce the chronic burden of symptoms, improve the patient experience, optimize the use of health resources, and redefine quality of life as a key, measurable outcome of medical care. Ultimately, this White Paper contributes to the evolution of medical thinking: from a disease-centered model to a medicine centered on function, people, and prevention.KEY MESSAGES
1. Chronic functional conditions are a major global health issue. Conditions with low mortality but high impact on daily functioning — such as dry eye and ocular surface diseases — affect hundreds of millions of people worldwide and constitute
PART I — BEFORE HIPPOCRATES
Medicine as Wisdom, Context, and Initiation1. The Beginning of Medicine Before Method
Before Medicine acquired methodology, protocols, and systematic recording, there was something deeper and more fundamental: a way of understanding man. In ancient Greek thought, treatment did not begin with the organ or the isolated pathology, but with the context of life in which the symptom emerged. Medicine, at this early stage, was not a technique. It was wisdom applied to care. This wisdom was not transmitted as information or memorized knowledge, but as initiation: a gradual education in observation, in the relationship between man and nature, and in understanding the balance between body, environment, and lifestyle. Health was not understood as the absence of symptoms, but as harmony.2. Chiron as the archetype of healer-teacher
At the heart of this pre-scientific Medicine is the figure of Chiron. Chiron is not a “historical figure” in the modern sense, but an archetype: the condensation of an entire way of medical thought and attitude towards man. In contrast to other mythological figures, Chiron: • does not heal with miracles, • does not promise immortality, • does not dominate. He teaches. His teaching includes: • observation of nature and its rhythms, • knowledge of herbs and natural remedies, • understanding of the body as a unified, dynamic system, • and, above all, an ethical attitude towards the suffering person. Healing, in the world of Chiron, is not an act of domination over the body, but an act of responsibility, relationship and respect.
3. Pelion and the cave: the place of therapeutic initiation
Pelion does not function simply as a geographical location, but as a symbolic space of therapeutic knowledge. In the cave of Chiron — a space between light and darkness — knowledge is not imposed; it is revealed. The choice of the cave is decisive, as: • it symbolizes silence and inner listening, • it presupposes a departure from the noise of the surface, • it signals the transition from the phenomenon to the essential. Medicine, in this phase, is not separated from philosophy and life. The therapist is first trained to see, before attempting to intervene. To understand before correcting. To respect before touching.4. The sacred triangle: Olympus – Pelion – Delphi
Pre-Hippocratic Medicine is part of a broader mental and spiritual framework, which can be symbolically attributed as a sacred triangle: • Olympus — law, order, cosmic principle • Pelion — nature, therapy, applied wisdom • Delphi — reason, judgment, decision Healing is born in Pelion, where nature and human experience meet. However: • it is given meaning by Olympus, that is, by the perception of a higher order, • and is interpreted through Delphi, where judgment and decision acquire reason. Medicine, thus, is neither arbitrary nor mechanistic. It is situated within a cosmic, natural and human order.5. Medicine as a way of life and not as a technique
In this context, illness: • is not considered a punishment, • nor a simple mechanical error. It is an indication of a disruption of balance. The role of the therapist is not to “fix” an isolated organ, but: • to understand the context, • to restore harmony, • to accompany the person in the recovery process. Medicine here touches the person not only physically, but also existentially. And this element will constitute the deepest foundation of all subsequent developments.6. What is preserved from pre-Hippocratic Medicine
Pre-Hippocratic Medicine could not develop into a global science. It needed a method, a language and the ability to reproduce knowledge. But he left something invaluable: • Medicine as a relationship, • treatment as care, • and man as a whole. This foundation is not canceled by scientific progress. On the contrary, it is the element that today we are called to reintegrate — not to return to the past, but to move forward fully into the future. Transitional connection. From Chiron and Pelion, Medicine will move to the next stage: to therapeutic practice as an organized institution, with Asclepius. There, wisdom will meet care and the patient’s experience will be placed at the center of the process.
PART II — ASCLEPIUS
From wisdom to therapeutic practice1. Asclepius as a transition from initiation to healing
If Chiron expresses Medicine as wisdom and initiation, Asclepius marks the transition to a new, decisive stage: organized therapeutic practice. Asclepius is not presented simply as a deity, but as a healer. His deification does not indicate distance from man; it indicates that healing is now recognized as the highest human function, worthy of respect and institutional protection. In the Asclepian world, Medicine ceases to be just knowledge and becomes an experience of care.2. The Asclepia: the first organized places of treatment
With Asclepius, Medicine gains space. The Asclepia were not temples in the narrow religious sense, but integrated therapeutic environments, scattered throughout the Greek world. In the Asclepia: • the patient does not come only for a symptom, • is not treated as a carrier of a disease, • but as a person in need of rehabilitation. The treatment included: • cleanliness and hygiene, • rest and rhythm, • nutrition and exercise, • mental peace, • and the constant presence of the therapist. Medicine becomes an institution of care, not a simple act of intervention.3. Sleep: healing through safety and tranquility
A central practice at the Asclepia was sleep: the patient entered a state of sleep in an environment of safety, purity and tranquility. Sleep should not be understood as a supernatural ritual. It was a process of: • deep discharge, • physical and nervous relaxation, • internal reorganization. In modern terms, we would say that: • the autonomic nervous system calms down, • inflammation decreases, • and the body gains the time it needs to return to balance. Treatment here is not imposed. The conditions are created for it to happen.4. The patient at the center of the therapeutic process
In the Asclepian model, the patient: • is not a passive recipient of instructions, • is not an object of treatment, • but an active participant. The therapeutic process: • respects the body’s time, • adapts to the needs of the person, • takes into account the environment, the mental state and the way of life. This element of care as a relationship will form the basis on which the scientific method will later be built.5. What did Asclepius offer to world medicine
The contribution of Asclepius is not scientific in the modern sense, but it is fundamental. He offered: • the first institution of organized therapy, • the therapeutic space as part of healing, • the continuous therapist-patient relationship, • the concept that healing is a process and not an instantaneous act. Without the Asclepian stage: • Medicine would have remained abstract wisdom, • or would have later evolved into an impersonal technique.6. The limits of the Asclepian model
Despite its power, the Asclepian model had clear limits: • it lacked a universal methodology, • it did not produce reproducible knowledge, • it could not be generalized beyond space and person. Treatment depended on: • the environment, • the therapist, • the patient’s experience. For Medicine to evolve into a universal science, the next step was needed.7. Transitional connection
Chiron’s wisdom gave meaning. Asclepius’ care gave experience. What was missing was: • systematic observation, • a common language, • the ability to diagnose, predict, and strategize treatment. This gap would be filled by Hippocrates.
PART III — HIPPOCRATES
The revolution of method1. The need for method
Medicine, as it evolved through Chiron and Asclepius, had already acquired wisdom and care. What it lacked, however, was method: a way of thinking that allowed for systematic observation, a common language, and the transmission of knowledge beyond place and person. At this historical point, Hippocrates appears, not as a mythical figure, but as a historical figure who introduces a radical cut. This cut is not technical. It is epistemological.2. The removal of the divine: a necessary act
Hippocrates’ most radical act was the removal of the supernatural from the interpretation of disease. Disease ceases to be attributed: • to divine punishment, • to demonic intervention, • to fatal necessity. It is treated as a natural phenomenon, which can: • be observed, • be described, • be understood. This abstraction was not a denial of meaning. It was the prerequisite for the universality of Medicine. Without it, Medicine could not become the common language of humanity.3. The birth of diagnosis
With Hippocrates, the concept of diagnosis is born for the first time. Not as a name for a disease, but as a process of understanding. Diagnosis means: • observation of the body over time, • correlation of symptoms, • understanding of the course. The doctor does not see a symptom in isolation. He sees the person within his disease.4. Prognosis: responsibility towards time
Along with the diagnosis, Hippocrates introduces prognosis. Prognosis is not a prediction in the oracle sense, but: • assessment of the course, • understanding of risks, • assuming responsibility towards the patient’s future. The doctor is not limited to the present. He assumes responsibility for how the situation will develop. This concept of prognosis establishes the ethics of Medicine.5. Treatment as a strategy
Treatment, in the Hippocratic world, ceases to be random or ritualistic. It becomes strategic. It includes: • choosing an appropriate intervention, • assessing time, • respecting the limits of the body. Medicine acquires a logical sequence: observe → understand → intervene. This pattern remains the core of clinical practice to this day.
6. What did Hippocrates offer to world medicine
Hippocrates’ contribution is unique and unrepeatable. He offered: • the method of systematic observation, • the distinction between disease and patient, • diagnosis, prognosis and therapeutic strategy, • the ability to teach and transmit medicine. Without Hippocrates: • there would be no modern clinical practice, • there would be no scientific medicine, • there would be no world medicine.7. The price of success
The Hippocratic revolution was life-saving. However, every great breakthrough has its price. The removal of the divine: • liberated knowledge, • but gradually removed the wisdom of the context. The method: • became stronger, • but began to operate often disconnected from the patient’s experience. The triad: • wisdom (Chiron), • care (Asclepius), • method (Hippocrates), gradually shrank into a unit.8. Transitional connection
Hippocrates did not cancel the past. He systematized it. The question that arises today is not whether Hippocrates was wrong. It is whether we have forgotten to preserve what came before. This question leads to the next part.
PART IV — WHAT WAS LOST AFTER
When the trinity became a unit1. From synthesis to the monopoly of method
The Hippocratic revolution was necessary and salutary. Thanks to it, Medicine acquired: • scientific language, • educational potential, • reproducibility, • global dissemination. However, its historical success gradually led to a monopoly of method. Method — from a tool — began to transform into an end in itself. Medicine became extremely capable of: • recognizing structural pathologies, • treating acute diseases, • intervening with precision. However, it began to have difficulty in: • understanding functional disorders, • listening to the patient when he “does not seem sick”, • embracing the experience of everyday discomfort.2. The contraction of the original triad
The original triad of Medicine: • Wisdom and context (Chiron), • Care and therapeutic experience (Asclepius), • Method and systematization (Hippocrates), was not lost by intention. It was shrunk by the excessive success of the third component. The method: • became more precise, • became faster, • became specialized. And within this success: • the context was weakened, • care became a process, • the person was often translated into a given.3. The birth of medical invisibility
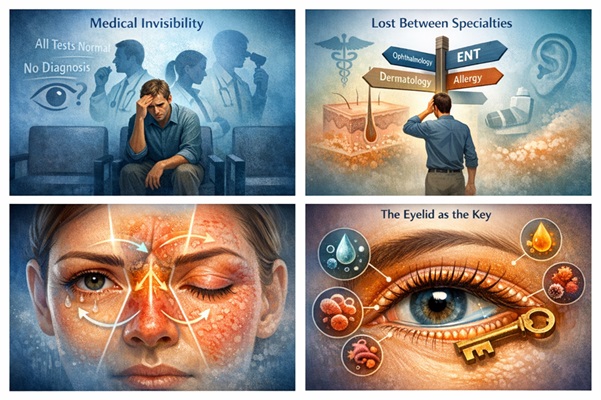
One of the most silent but profound results of this evolution is what can be called medical invisibility. It concerns the patient who: • has symptoms, • experiences discomfort, • but does not meet the criteria for a clear diagnosis. In this context, phrases such as: • “you have nothing”, • “the tests are clear”, • “no pathology is seen”. The method has worked correctly. However, the person has not been relieved.4. The patient who is lost between specialties
The increasing specialization — although necessary — has created another phenomenon: the patient who moves from specialty to specialty without an overall framework. Each specialist: • examines his own field excellently, • rules out serious pathology, • but does not take on the whole. The result is not medical negligence. It is a structural gap. The patient: • gets tired, • doubts himself, • begins to believe that he is “exaggerating” or that “the problem is psychological”.5. When technique outweighs relationship
In the modern health system, time: • is limited, • fragmented, • measured. The therapist-patient relationship: • shrinks, • is replaced by checklists, • is translated into codes. Medicine becomes extremely effective, but often less present. And this is precisely where the modern paradox appears: never has Medicine been so powerful — and never have so many people felt so incomprehensible.6. It is not a failure — but a transition
This chapter is not a criticism of modern Medicine. It is a diagnosis of a historical transition. Medicine: • did what it had to do, • went as far as it should, • but reached a point that requires recomposition. Not a return to the past, but the reinstatement of what was lost within a modern, scientific framework.7. Transitional connection
The question that arises is not theoretical. It is absolutely practical: What happens to the patient who suffers, but does not “fit” into a diagnosis? The answer begins to emerge in the next part, through a modern, everyday clinical example.
PART V — THE MODERN EXAMPLE
When the patient has symptoms but “has nothing”1. The patient who tears and finds no answer
A person comes to the doctor with complaints of: • tearing, • irritation, • burning or foreign body sensation, • fluctuations in vision, • eye fatigue. The tests: • do not reveal serious structural pathology, • visual acuity is good, • there is “nothing to worry about.” The answer he receives is often reassuring — but incomplete: “You have nothing.” And yet, the patient does not feel well.2. The experience of medical wandering
A familiar path follows: • changing ophthalmologists, • visiting an allergist, • examination by an ENT specialist, • alternating eye drops and antihistamines. Each specialist examines his own field correctly. No one makes mistakes. And yet, the problem persists. The patient begins to: • get tired, • doubt himself, • wonder if he is “imagining it.” Here medical invisibility is born in its everyday form.3. Symptom-finding discrepancy as a recognized phenomenon
The discrepancy between symptoms and objective findings is now a recognized phenomenon in diseases of the ocular surface. Clinical researchers have noted that dry eye is often underdiagnosed, as the patient’s experience precedes and is not always reflected in available diagnostic tests. This leads not only to delayed diagnosis, but also to a sense of deconstruction of the patient’s experience, who often feels “not taken seriously” (6–8).4. What the science shows—and why it matters
In parallel with this experience, the scientific literature clearly shows: • an increase in dry eye, • an explosive incidence of meibomian gland dysfunction (MGD), • a high incidence of blepharitis, • a close association with allergic conditions (1–5, 9–12). Studies show that chronic low-grade inflammation of the ocular surface: • affects tear film stability, • causes reflex tearing, • reduces the quality of vision even with “good visual acuity” (1–4). The problem exists. It is simply not always visible by the classic criteria.5. When the eyes, nose, and skin speak the same language
Allergic conjunctivitis is rarely isolated. It is often part of a single syndrome: allergic rhinoconjunctivitis, where: • the eyes, • the nasal cavity, • and the skin, participate in a common inflammatory response (17–18). Furthermore, the naso-ocular reflex explains how nasal irritation can cause: • tearing, • itching, • redness, even without primary ocular disease (19–20). The symptom, therefore, does not belong to a specialty. It belongs to an interface.6. The eyelid as a lost key
At the center of this interface is the eyelid: • skin, • eyelashes, • glands, • microbiome. Its dysfunction: • destabilizes the tear film, • increases evaporation, • enhances inflammation (9–12). Dermatological literature has shown that conditions such as rosacea: • often show ocular involvement, • and can manifest mainly with blepharitis (13–14). The eyelid is not just a “periphery of the eye”. It is a functional regulator of ocular comfort.7. How the patient experiences this dimension
When there is no clear diagnosis: • the patient feels unheard, • has difficulty explaining their problem, • often accepts the discomfort as “normal”. The social and psychological impact is real: • reduced concentration, • fatigue, • avoidance of activities, • reduced quality of life (21–22). And yet, this burden is not captured in a single examination.8. Transitional connection
This example is not about a “gray zone” of medicine. It concerns millions of people. The answer is not found: • in more eye drops, • nor in fragmented visits. It lies in the need for a unifying scientific framework that sees: • the eye, • the skin, • the nose, as a single operating system. This framework begins to take shape in the next part.
PART VI — THE BIRTH OF DERMOOPHTHALMOLOGY
The Reunification of the Triad in Modern Medicine
1. Why a New Unifying Framework Was Needed
Dermoophthalmology was not born as a theoretical concept. It was born in response to a clinical void. A void that arose when:
• the symptoms were present,
• the tests appeared “normal,”
• and the patient remained without substantial relief.
Modern Medicine has excellent diagnostic and therapeutic tools. What was missing was not the technique — but the connection.
Dermo-Ophthalmology proposes a unifying scientific framework that:
• does not negate existing specialties,
• does not compete with Ophthalmology or Dermatology,
• but focuses on their functional meeting point.
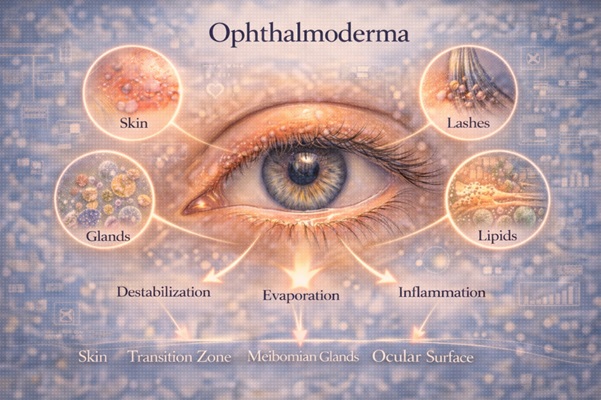
2. Ophthalmoderma
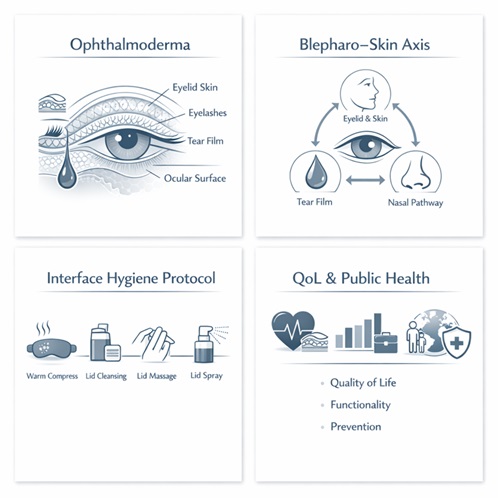
In Dermo-Ophthalmology, the term Ophthalmoderma is used to describe the single functional domain formed by the eyelid skin, the skin-mucosal transition zone, the eyelashes, the meibomian glands, and the ocular surface. It is an interface zone where dermatological, microbiological, immunological, and mechanical factors coexist and regulate tear film stability, visual comfort, and quality of vision (1–5, 9–12). The demarcation of the domain as “Ophthalmoderma” allows for the systematic description and clinical evaluation of an area where symptoms often precede classical objective findings. The eyelid as a central regulator of the Ophthalmoderm The eyelid: • is skin with particular anatomical and functional characteristics, • bears eyelashes and follicles, • houses the meibomian glands, • regulates the lipid layer of the tear film (9–12). Its dysfunction: • destabilizes the ocular surface, • increases tear evaporation, • triggers chronic low-grade inflammation (1–4, 9–12). The eyelid is not just a “periphery of the eye”. It is a key regulator of ocular comfort and quality of vision.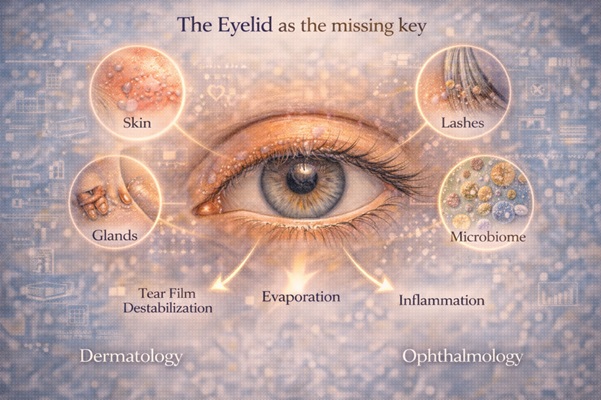
3. The Blepharo–Skin Axis: skin and eye as a single system
Dermo-Ophthalmology introduces the concept of the Blepharo–Skin Axis: a functional continuity between:
• the skin of the eyelids,
• the eyelashes,
• and the ocular surface.
Dermatological diseases such as:
• rosacea,
• seborrheic dermatitis,
• and skin barrier disorders,
can manifest primarily with ocular symptoms (13–14).
At the same time, modern research has shown that skin barrier disruption:
• promotes chronic inflammation,
• affects the microbiome,
• and destabilizes adjacent functional interfaces (15–16).
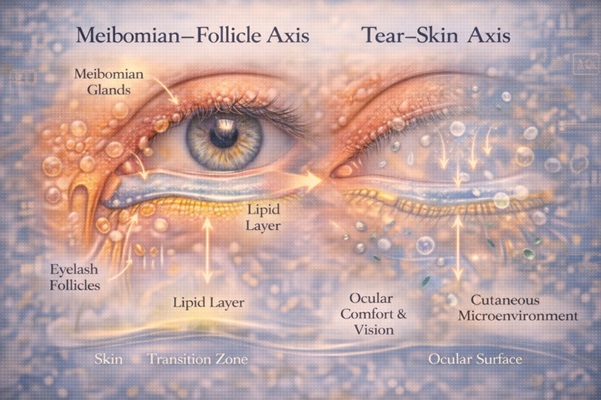
4. Meibomian–Follicle Axis and Tear–Skin Axis
Dermo-ophthalmology is not limited to a single axis. It describes a network of functional axes, including:
• Meibomian–Follicle Axis
→ connection of meibomian glands and eyelash follicles
→ regulation of the lipid layer and inflammation (9–12)
• Tear–Skin Axis
→ interaction of tear film with the dermal microenvironment
→ evaporation, ocular comfort and quality of vision (1–5)
These axes explain why:
• eyes can tear but be functionally “dry”,
• visual acuity can be good but comfort is poor,
• and treatment without hygiene fails in the long term (1–5, 9–12).
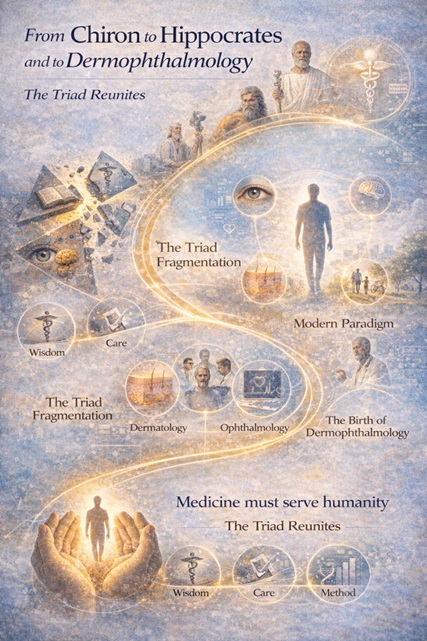
5. Reuniting the triad in modern terms
Dermophthalmology reunites, in modern scientific language, the original triad of Medicine:
• Wisdom / Context (Chiron) → understanding of interfaces and quality of life
• Care / Action (Asclepius) → daily hygiene, environment, prevention
• Method (Hippocrates) → diagnosis, prognosis, documentation
This is not a return to the past. This is a synthesis in the present.
6. Collaboration of specialties, not loss of roles
Dermophthalmology:
• does not remove responsibilities from the ophthalmologist,
• does not replace the dermatologist or ENT,
• does not create competition between specialties.
On the contrary:
• facilitates collaboration,
• improves clinical understanding,
• reduces the patient’s medical wandering.
The doctor does not “lose a role”. He gains context.
7. Transitional connection
Dermophthalmology is not the end of the journey. It is the point where Medicine:
• remembers its origins,
• and responds to the needs of today.
The next step concerns how this synthesis is translated into daily clinical practice: in hygiene, prevention and a change in mentality.
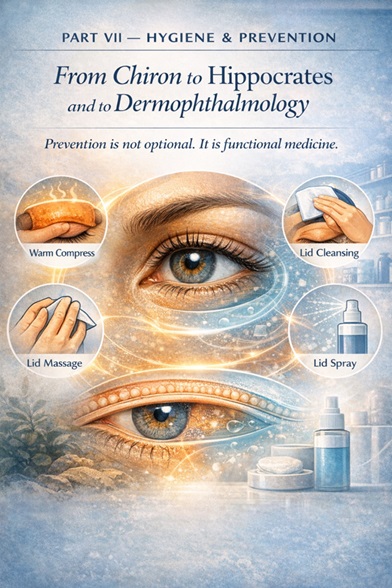
PART VII — HYGIENE & PREVENTION
When care becomes a daily medical practice
1. Hygiene as the foundation of modern prevention
Hygiene is one of the oldest and at the same time most modern pillars of Medicine. Before any pharmaceutical or invasive procedure, Medicine has always relied on prevention through care.
In modern times, hygiene:
• is not a simple recommendation,
• is not an auxiliary measure,
• but a documented medical intervention (9–12).
Especially in chronic conditions of low intensity but high frequency, hygiene functions as a stabilizing mechanism.
2. Why we wash/care for what we consider important
Humans have incorporated hygiene into critical parts of the body:
• the skin,
• the hair,
• the teeth.
Daily hygiene:
• prevents the accumulation of microbial load,
• protects the barrier,
• maintains function.
The eyes, however, and especially the eyelids, have traditionally been excluded from this logic. Not because they do not need it, but because they have not been recognized as a functional interface.
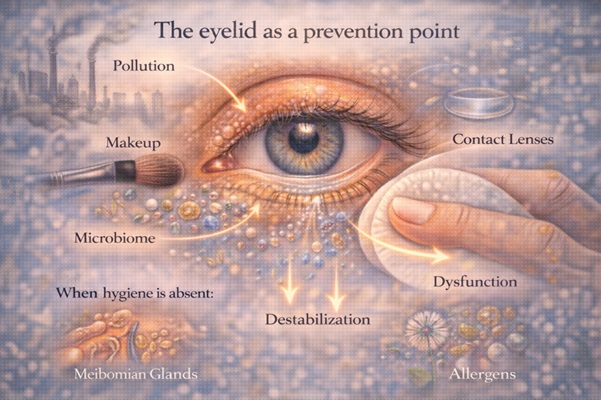
3. The eyelid as a point of prevention
The eyelid:
• comes into daily contact with pollutants,
• hosts a microbiome,
• is exposed to makeup, contact lenses, allergens and environmental factors.
When hygiene is absent:
• the microenvironment is disrupted,
• the meibomian glands malfunction,
• the tear film is destabilized (9–12).
Prevention here is not about avoiding disease in the future. It is about maintaining functionality in the present.
4. Heat, cleansing, massage, spray and functional restoration
Modern clinical practice shows that: • controlled heat (~40°C) liquefies lipid secretions, • decongests the eyelids and improves the quality of vision, • cleansing the eyelid margin reduces the inflammatory load, • eyelid massage improves microcirculation in the area, • consistency in care is crucial (9–12). Eyelid hygiene: • does not replace treatment, • but supports and stabilizes it. Just as oral hygiene does not replace dentistry, eyelid hygiene does not replace ophthalmology — it complements it.5. From treatment to prevention: a paradigm shift
The old health model was based on the logic: “I let something break down and then I fix it.” In the eyes, this model is problematic: • they are not replaced, • chronic dysfunction accumulates, • delay costs quality of vision and life. Prevention on the ocular surface: • is not an exaggeration, • is a wise investment.6. Hygiene as a mindset, not a product
The essence of hygiene is not found in a specific preparation. It is found in the mindset of care. When hygiene: • is integrated into everyday life, • is explained with scientific clarity, • is guided by the doctor, the patient: • gains control, • reduces insecurity, • ceases to be a passive recipient of treatments. Medicine becomes collaborative.7. Transitional connection
Hygiene and prevention are not the end of Medicine. It is the return of Medicine to everyday life. This transition requires: • a change in mindset, • a redefinition of the role of the physician, • and the integration of quality of life at the center of care. This change constitutes the final part.
PART VIII — CHANGE OF MINDSET
Quality of Life, Public Health and the Future of Medicine
1. From the Absence of Disease to Quality of Life
For much of its history, medicine has defined health as the absence of disease. This definition has been practical and necessary, but today it is proving to be inadequate.
Contemporary reality shows that:
• millions of people do not suffer from a clear disease,
• but live with chronic discomfort,
• reduced functionality,
• and limited quality of life.
Quality of Life (QoL) is no longer a subjective concept. It is a measurable indicator of health, inextricably linked to the functional state of the person (21–24).
In ophthalmology, this is particularly evident: good visual acuity does not guarantee good quality of vision. Visual acuity, although a key indicator, is not sufficient to capture the patient’s overall visual experience. As has been emphasized in the current clinical literature, dry eye/blepharitis is primarily a quality of life disease, with symptoms such as burning, tearing, fatigue, and intermittent blurring, which affect daily functioning regardless of visual acuity (6–8, 21–22).
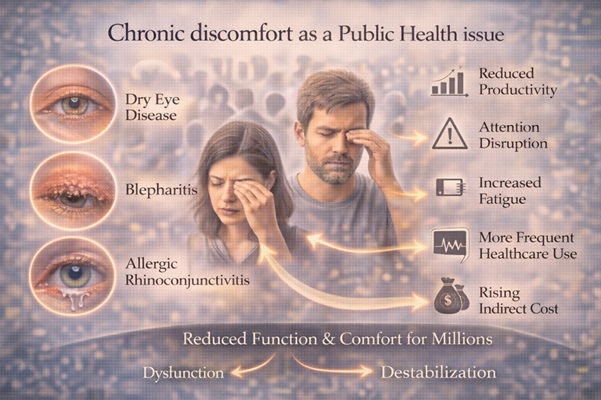
2. Chronic discomfort as a public health issue
Diseases such as:
• dry eye,
• blepharitis,
• allergic rhinoconjunctivitis,
are not directly life-threatening. However, they threaten the daily functioning of millions of people.
At the population level, this translates into:
• reduced productivity,
• distraction,
• increased fatigue,
• increased use of health services,
• and increasing indirect costs (23–28).
The modern approach to public health recognizes that chronic conditions with low mortality but high impact on functioning are a critical priority (23–27). Ocular comfort and functional vision fall into this category.
3. The economics of prevention
The shift from treatment to prevention is not only anthropocentric. It is also economically necessary.
Prevention:
• reduces relapses,
• limits drug dependence,
• reduces the need for repeat medical visits (23–28).
In chronic quality of life conditions, interventions:
• low cost,
• high compliance,
• daily application,
have a high return on investment (ROI) for health systems. Eyelid hygiene fits precisely into this model: not as a crisis treatment, but as a stabilizing strategy (9–12).
4. The new role of the physician
In this new context, the role of the physician is evolving.
The physician:
• is not limited to diagnosis,
• is not limited to prescribing,
• but acts as a guide for prevention and care.
The doctor-patient relationship:
• becomes collaborative,
• is based on education,
• enhances self-management with scientific guidance (29–30).
This role:
• does not weaken scientific authority,
• deepens it.
5. Medicine of interfaces
Dermophthalmology is an example of a broader shift: Medicine of interfaces.
A medicine that:
• does not see organs in isolation,
• but systems in constant interaction,
• focuses on function, not just structure.
The eye, skin, and nasal cavity are not separate realities. They constitute a single functional field with a direct impact on quality of life (17–22).
6. Prevention as modern wisdom
In the eyes, more than any other organ, prevention is not an option — it is a necessity.
The eyes:
• are not replaceable (like teeth),
• transmit 80% of our information,
• determine autonomy and social functioning.
The acceptance of chronic discomfort as a “normal state” is a silent resignation that modern Medicine must review.
7. Final synthesis — the return of the triad
Global Medicine:
• began as a triad,
• evolved into a unit,
• and today is called upon to reintegrate the synthesis.
Not to return to the past. But to respond to the needs of the present.
• Wisdom and context
• Care and practice
• Method and science
Dermophthalmology is no exception. It is a model of this evolution. The recognition of the subjective experience of the patient does not weaken scientific Medicine; on the contrary, it complements it. The integration of patient-reported outcomes into clinical decision-making is a crucial step for a modern, human-centered approach to chronic functional diseases (29–30).
Epilogue
Medicine was not born as a technique. It was born as care, wisdom, and responsibility towards man. The challenge of the 21st century is not to do more. It is to see better. And this, perhaps, is the deepest meaning of Medicine — from Chiron to the present.
REFERENCES
I. ΘΕΜΕΛΙΩΣΗ ΟΦΘΑΛΜΟΛΟΓΙΑΣ & ΟΦΘΑΛΜΙΚΗΣ ΕΠΙΦΑΝΕΙΑΣ
1. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II Definition and Classification Report. Ocul Surf. 2017;15(3):276–283.
2. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II Management and Therapy Report. Ocul Surf. 2017;15(3):575–628.
3. Baudouin C, Irkec M, Messmer EM, et al. Clinical impact of inflammation in dry eye disease: proceedings of the ODISSEY group meeting. Acta Ophthalmol. 2018;96(2):111–119.
4. Baudouin C, Messmer EM, Aragona P, et al. Revisiting the vicious circle of dry eye disease: a focus on the pathophysiology of meibomian gland dysfunction. Br J Ophthalmol. 2016;100(3):300–306.
5. Stapleton F, Alves M, Bunya VY, et al. TFOS DEWS II Epidemiology Report. Ocul Surf. 2017;15(3):334–365.
6. McDonald M, Pflugfelder SC, Palay DA, et al. Understanding the unmet needs of patients with dry eye disease. Ophthalmology Management. 2016;20(7):30–36.
7. McDonald M. Dry eye disease: the disconnect between signs and symptoms. EyeWorld. 2018;23(4):28–31.
8. McDonald M. Why dry eye is a quality-of-life disease, not just an ocular surface disorder. Ophthalmology Times. 2019;44(6):18–21.
II. ΜΕΪΒΟΜΙΑΝΟΙ ΑΔΕΝΕΣ – ΒΛΕΦΑΡΑ – ΥΓΙΕΙΝΗ
9. Nichols KK, Foulks GN, Bron AJ, et al. The International Workshop on Meibomian Gland Dysfunction: Executive Summary. Invest Ophthalmol Vis Sci. 2011;52(4):1922–1929.
10. Blackie CA, Solomon JD, Greiner JV, et al. The relationship between dry eye symptoms and lipid layer thickness. Cornea. 2009;28(7):789–794.
11. Arita R, Mizoguchi T, Kawashima M, et al. Meibomian gland dysfunction and dry eye are similar but different based on a population-based study. Ophthalmology. 2019;126(7):974–981.
12. Liu J, Sheha H, Fu Y, et al. Update on eyelid margin diseases and management. Ocul Surf. 2019;17(4):567–584.
III. ΔΕΡΜΑΤΟΛΟΓΙΑ – ΟΦΘΑΛΜΟΔΕΡΜΑ – ROSACEA
13. Tan J, Blume-Peytavi U, Ortonne JP, et al. An observational cross-sectional survey of rosacea: clinical associations and severity. J Am Acad Dermatol. 2013;69(5):S57–S65.
14. Tan J, Almeida LMC, Bewley A, et al. Rosacea: current state of epidemiology. J Am Acad Dermatol. 2016;75(4):567–579.
15. Gallo RL, Bernard JJ. Innate immune sensors stimulate inflammatory responses to ultraviolet radiation. Nat Rev Immunol. 2014;14(10):678–686.
16. Gallo RL. Human skin is the largest epithelial surface for interaction with microbes. J Invest Dermatol. 2017;137(6):1213–1214.
IV. ΩΤΟΡΙΝΟΛΑΡΥΓΓΟΛΟΓΙΑ – ΑΛΛΕΡΓΙΑ – NASO-OCULAR AXIS
17. Bousquet J, Khaltaev N, Cruz AA, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 update. Allergy. 2008;63 Suppl 86:8–160.
18. Bousquet J, Schünemann HJ, Togias A, et al. Next-generation ARIA care pathways for allergic rhinitis and asthma. Allergy. 2019;74(8):1552–1561.
19. Baraniuk JN. Neurogenic mechanisms in rhinosinusitis. Curr Allergy Asthma Rep. 2011;11(3):217–224.
20. Baraniuk JN, Merck SJ. Neuroregulation of human nasal mucosa. Ann N Y Acad Sci. 2009;1170:604–609.
V. ΠΟΙΟΤΗΤΑ ΖΩΗΣ (QoL) & ΛΕΙΤΟΥΡΓΙΚΗ ΥΓΕΙΑ
21. Uchino M, Schaumberg DA. Dry eye disease: impact on quality of life and vision. Curr Ophthalmol Rep. 2013;1(2):51–57.
22. Miljanović B, Dana R, Sullivan DA, Schaumberg DA. Impact of dry eye syndrome on vision-related quality of life. Am J Ophthalmol. 2007;143(3):409–415.
23. World Health Organization. WHOQOL: Measuring Quality of Life. Geneva: WHO; 1997.
24. World Health Organization. International Classification of Functioning, Disability and Health (ICF). Geneva: WHO; 2001.
VI. ΔΗΜΟΣΙΑ ΥΓΕΙΑ – ΧΡΟΝΙΑ ΝΟΣΗΜΑΤΑ – ΠΡΟΛΗΨΗ
25. World Health Organization. Innovative Care for Chronic Conditions: Building Blocks for Action. Geneva: WHO; 2002.
26. World Health Organization. Preventing chronic diseases: a vital investment. Geneva: WHO; 2005.
27. World Health Organization. Global Health Estimates: Disease burden by cause, age, sex, by country and by region. Geneva: WHO; 2018.
28. Nolte E, McKee M. Caring for people with chronic conditions: A health system perspective. Maidenhead: Open University Press; 2008.
VII. ΣΥΝΘΕΣΗ – ΑΝΘΡΩΠΟΚΕΝΤΡΙΚΗ ΙΑΤΡΙΚΗ
29. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196(4286):129–136.
30. Berwick DM. What ‘patient-centered’ should mean: confessions of an extremist. Health Aff. 2009;28(4):w555–w565.
ABBREVIATIONS
• WOD: World Organization of Dermophthalmology
• WHO: World Health Organization
• QoL: Quality of Life
• PROs: Patient-Reported Outcomes
• MGD: Meibomian Gland Dysfunction
• TFOS DEWS II: Tear Film & Ocular Surface Society — Dry Eye Workshop II
• ARIA: Allergic Rhinitis and its Impact on Asthma