Institutional Statement
The Dermophthalmology framework was developed by the scientific team of the World Organization of Dermophthalmology (WOD) under the conceptual initiation of John Tsakalos. It does not constitute a new medical specialty. It proposes an integrative systems framework for understanding ocular surface stability as a functional bio-interface.
Abstract
Current ocular surface disease models effectively describe structural pathology and inflammatory markers. However, a substantial population experiences functional visual instability—fluctuating clarity, fatigue, environmental intolerance—without overt clinical findings.
Dermophthalmology proposes a systems-based framework in which the ocular surface is understood as part of a continuous epithelial–cutaneous interface termed the Ophthalmoderma, integrating:
- Eyelid skin biology
- Meibomian gland lipid dynamics
- Tear film physiology
- Microbiome ecology
- Environmental exposure
- Neuro-sensory processing
Central to this model is the concept of the Ophthalmodermal Barrier, describing the integrated mechanical, immune, microbial, and optical interface between environment and visual processing. Rather than redefining disease, this framework reorganizes fragmented knowledge into a coherent systems paradigm centered on functional stability.
1. The Fragmentation Problem in Ocular Surface Medicine
Ophthalmology traditionally evaluates:
• Corneal integrity
• Tear volume metrics
• Inflammatory markers
• Visual acuity
Dermatology evaluates:
• Skin barrier function
• Microbial balance
• Inflammatory reactivity
Otolaryngology evaluates:
• Nasal airflow
• Mucosal inflammation
• Environmental filtering
Neurology evaluates:
• Sensory processing
• Central sensitization
• Cortical load
Environmental medicine evaluates:
• Humidity
• Pollution
• Allergen exposure
The patient experiences none of these separately. The patient experiences visual stability. Dermophthalmology functions as a systems integrator of these domains.
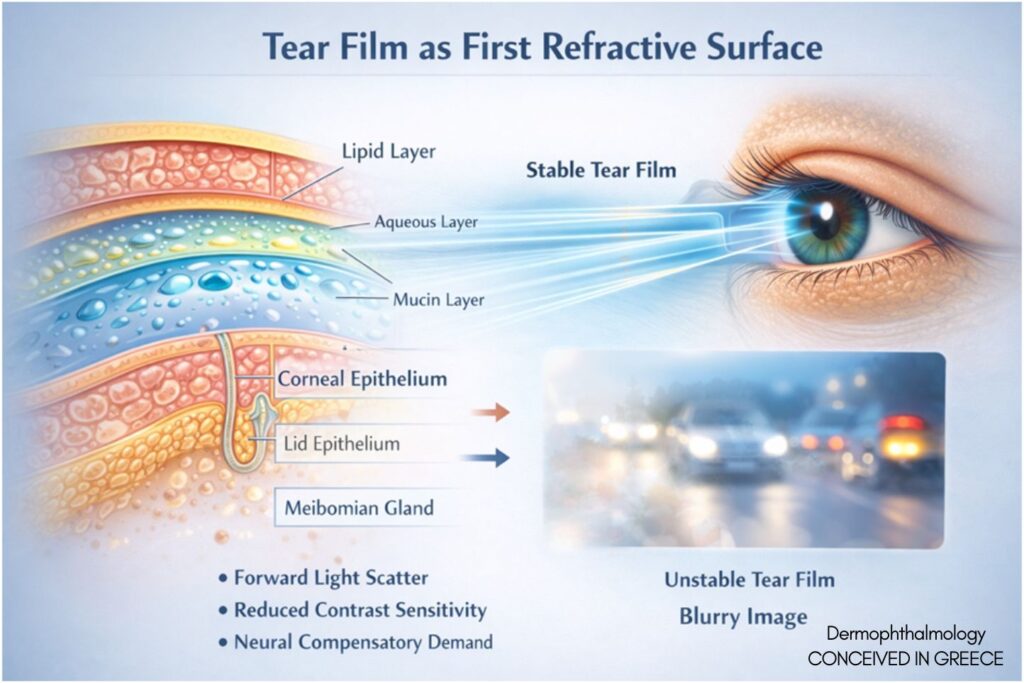
2. The Tear Film as the First Refractive Surface
The tear film constitutes the first refractive interface of the optical system (Bron et al., 2004; Nichols et al., 2005).
Instability leads to:
• Increased forward light scatter
• Reduced contrast sensitivity
• Micro-fluctuations in image quality
• Increased neural compensatory demand
This reframes tear film dynamics from lubrication mechanics to optical interface biology.
________________________________________
3. The Ophthalmoderma Continuum
Eyelid skin and ocular surface epithelium share:
• Ectodermal embryologic origin
• Immune regulatory pathways
• Barrier architecture principles
• Microbiome interaction patterns
(Barabino & Dana, 2004; Knop et al., 2011)
The Ophthalmoderma describes this continuous epithelial–cutaneous unit as a functional system rather than separate anatomical territories.
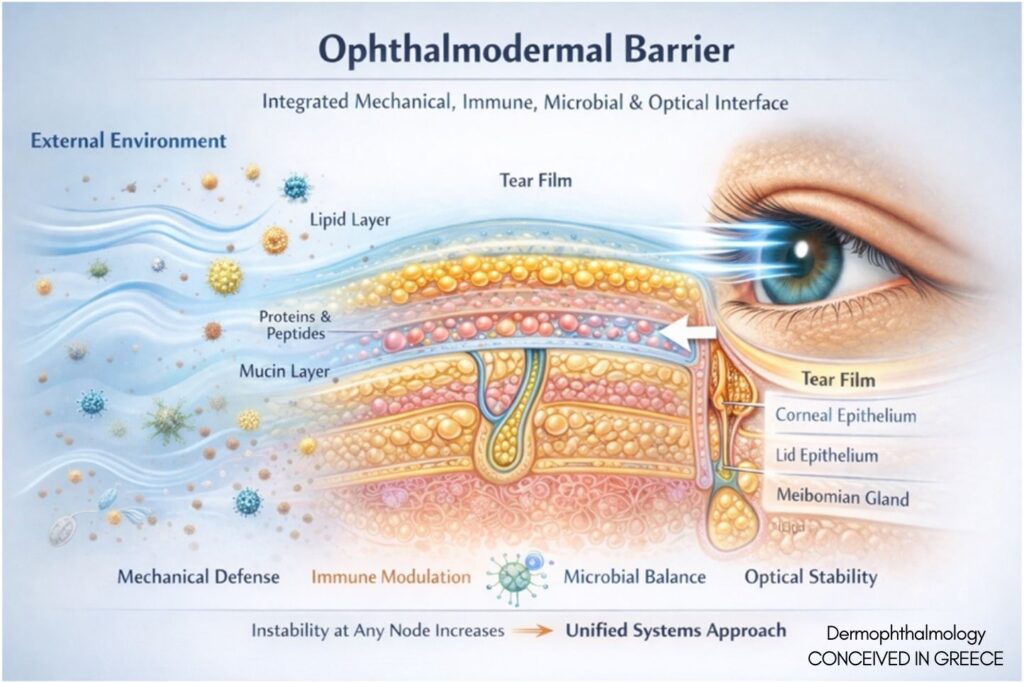
4. The Ophthalmodermal Barrier
Analogous to:
• The skin barrier
• The gut barrier
• The blood-brain barrier
The Ophthalmodermal Barrier represents the integrated:
• Blink-mediated mechanical defense
• Lipid layer stabilization
• Immune modulation
• Microbial equilibrium
• Environmental buffering capacity
Barrier instability may manifest as functional dysregulation before structural disease.
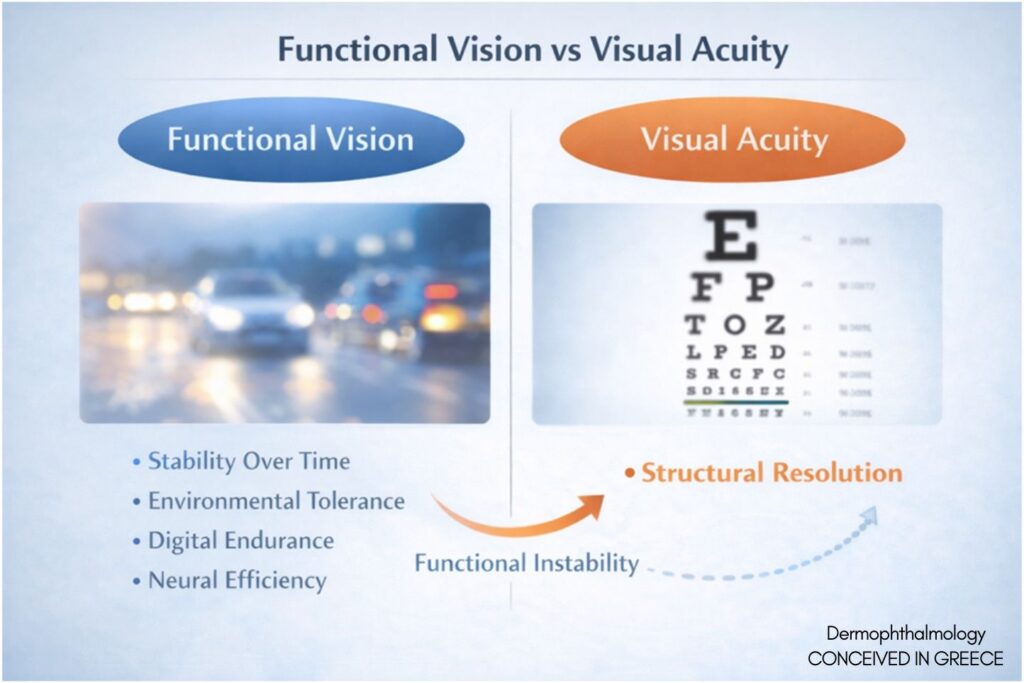
5. Functional Vision Beyond Visual Acuity
Visual acuity measures structural resolution. Functional vision includes:
• Stability over time
• Environmental tolerance
• Digital endurance
• Neural efficiency
(Tsubota, 2018; Craig et al., 2017)
Functional instability represents early systems dysregulation.

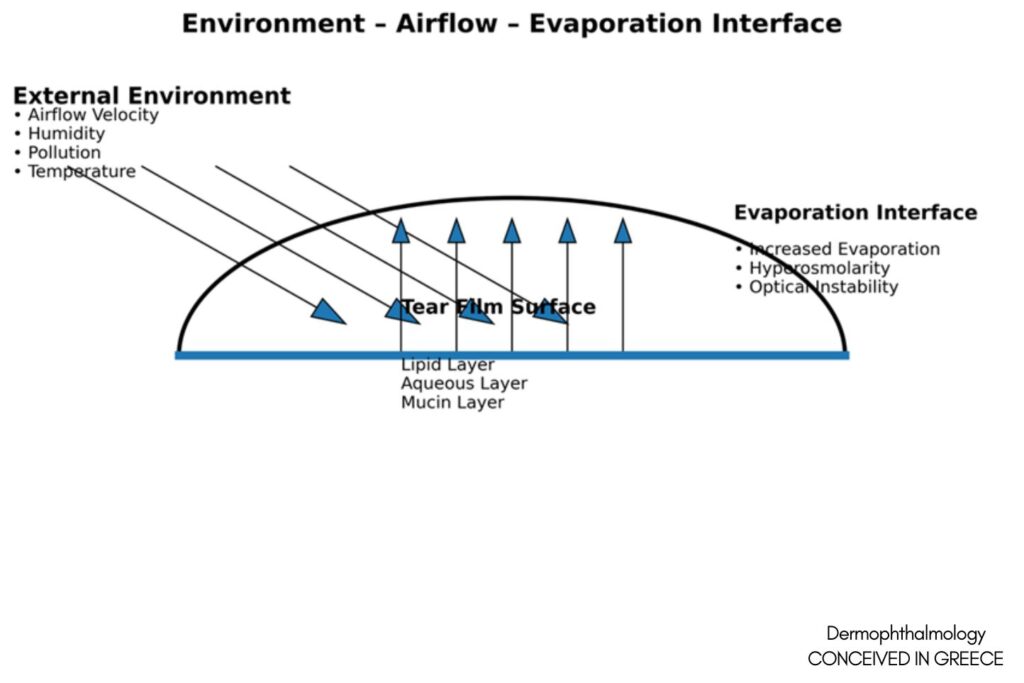
6. Environmental and Airflow Contributions
The ocular surface is uniquely exposed. Evaporation rate depends on:
• Humidity
• Airflow velocity
• Lipid layer integrity
(TFOS DEWS II Environmental Report, 2017)
The Nose–Airflow–Eye interface suggests otolaryngologic contributions to tear film stability. Chronic nasal inflammation and altered airflow patterns may increase evaporation and surface stress.
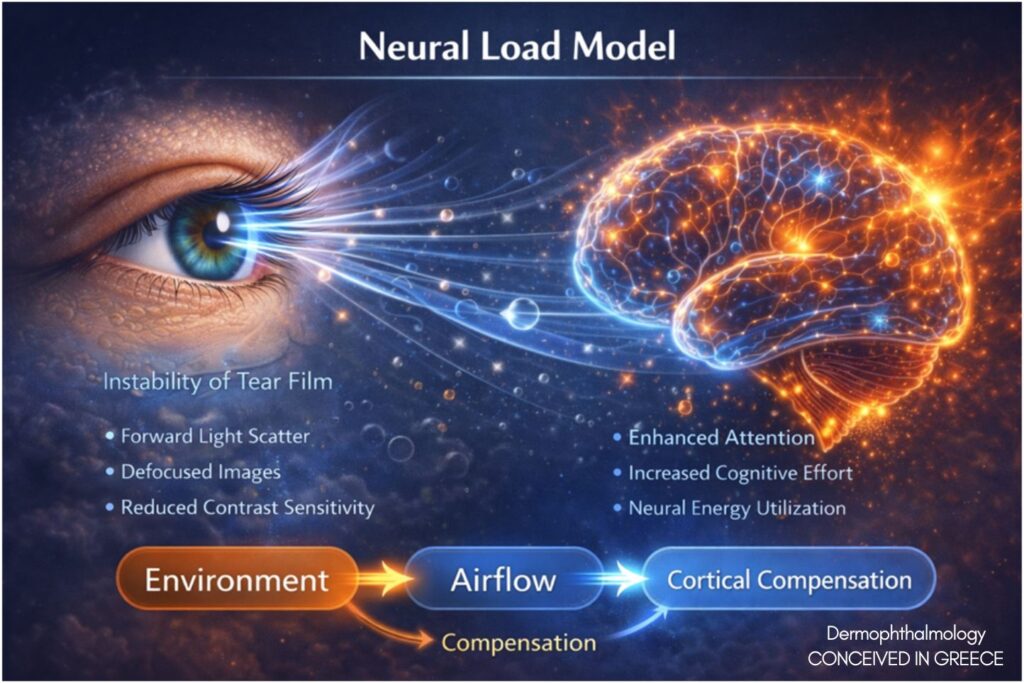
7. Neural Load and Sensory Processing
Unstable optical input increases:
• Sensory noise
• Cortical processing demand
• Visual fatigue
(Goadsby et al., 2017)
The brain does not originate dysfunction; it compensates for unstable input. Dermophthalmology emphasizes input stabilization rather than neural suppression.
________________________________________
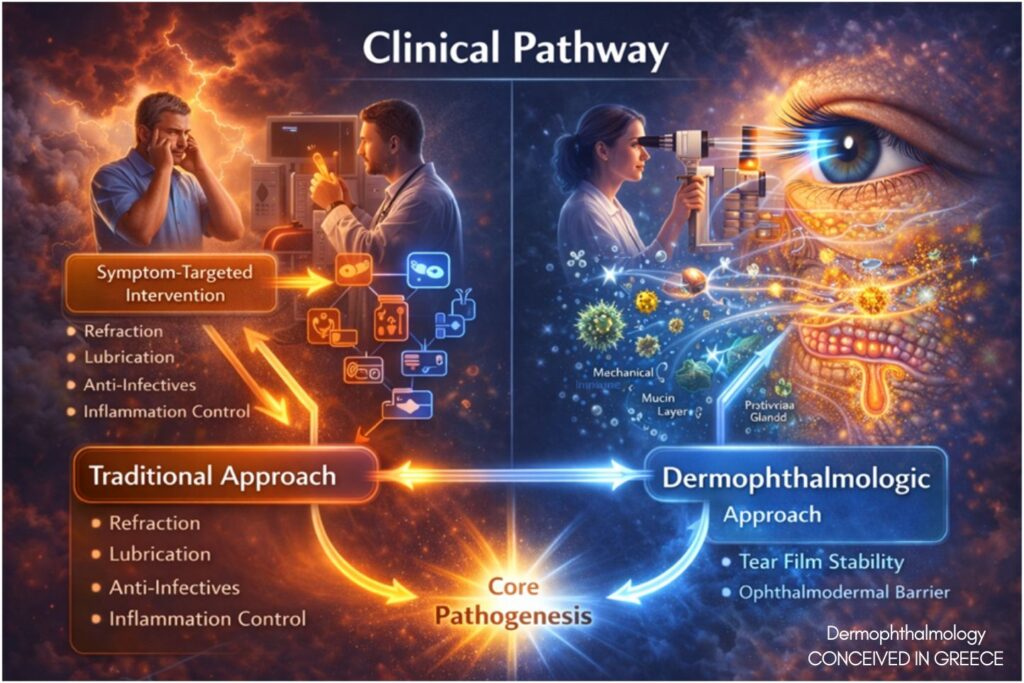
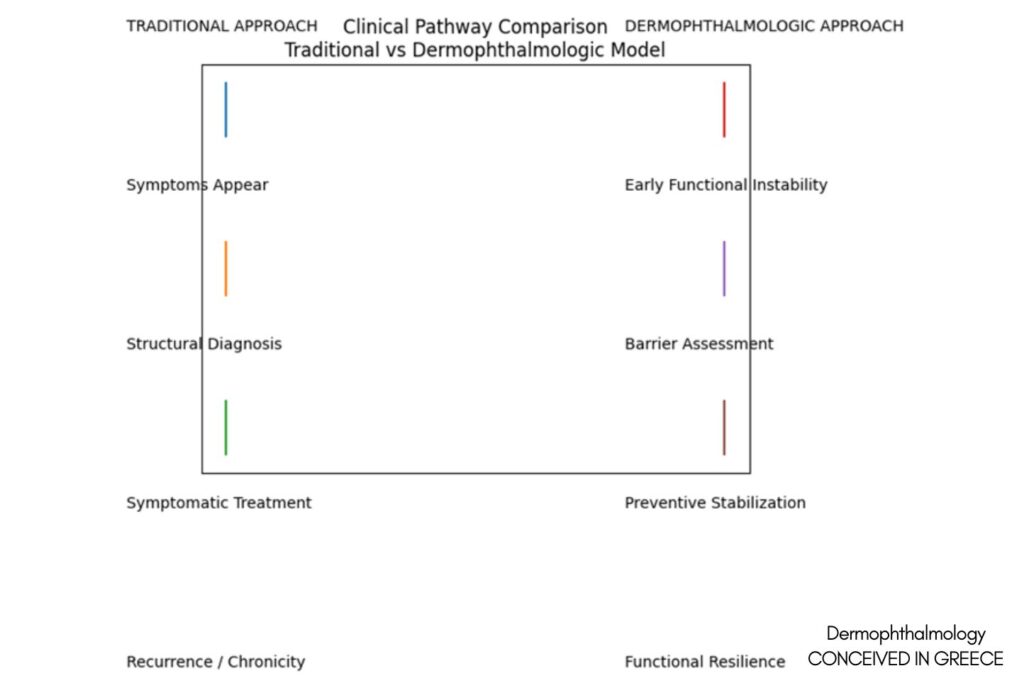
8. Clinical Implications
The framework supports:
• Early functional intervention
• Preventive stabilization
• Interdisciplinary collaboration
• Reframing of “idiopathic discomfort”
It does not replace guidelines. It contextualizes them.
________________________________________
9. Public Health Implications
Digital exposure, reduced blink rate, climate-controlled environments, and urban pollution create chronic low-grade instability. Functional ocular resilience becomes a public health issue. This aligns with WHO definitions of health as functional well-being.
________________________________________
10. Translational and Applied Clinical Considerations
Within this framework, dermophthalmologic clinical strategies aim to:
• Support eyelid surface hygiene
• Stabilize lipid layer dynamics
• Modulate low-grade inflammatory load
• Preserve Ophthalmodermal Barrier integrity
These principles are framework-driven rather than product-driven. Certain clinical protocols developed within the Ophthalmogen platform have been designed in alignment with dermophthalmologic stabilization principles. These represent translational applications of the conceptual model, not its definition.The framework precedes and informs the protocol.
________________________________________
11. Limitations
This framework:
• Is conceptual and integrative
• Requires longitudinal validation
• Does not substitute diagnostic criteria
• Does not replace established disease classification systems
Future empirical validation is required to quantify barrier instability biomarkers.
12. Future Research Directions
• Real-world tear film dynamics measurement
• Functional vision quantification tools
• Microbiome–environment interaction mapping
• Airflow modeling and ocular surface evaporation
• Neural load quantification in optical instability
13. Scientific and Clinical Significance
The significance of Dermophthalmology lies not in the introduction of new biological entities, but in the systemic reorganization of existing evidence into a unified functional paradigm. This framework:
• Addresses the gap between structural pathology and functional symptoms
• Integrates fragmented specialties under a common bio-interface model
• Repositions tear film instability as an early systems signal
• Provides a preventive logic aligned with digital-era environmental realities
Dermophthalmology offers:
• A translational bridge between ophthalmology and dermatologic barrier science
• A systems-level explanation for functional visual instability
• A public health-relevant reframing of ocular surface resilience
It represents conceptual integration rather than specialty creation.
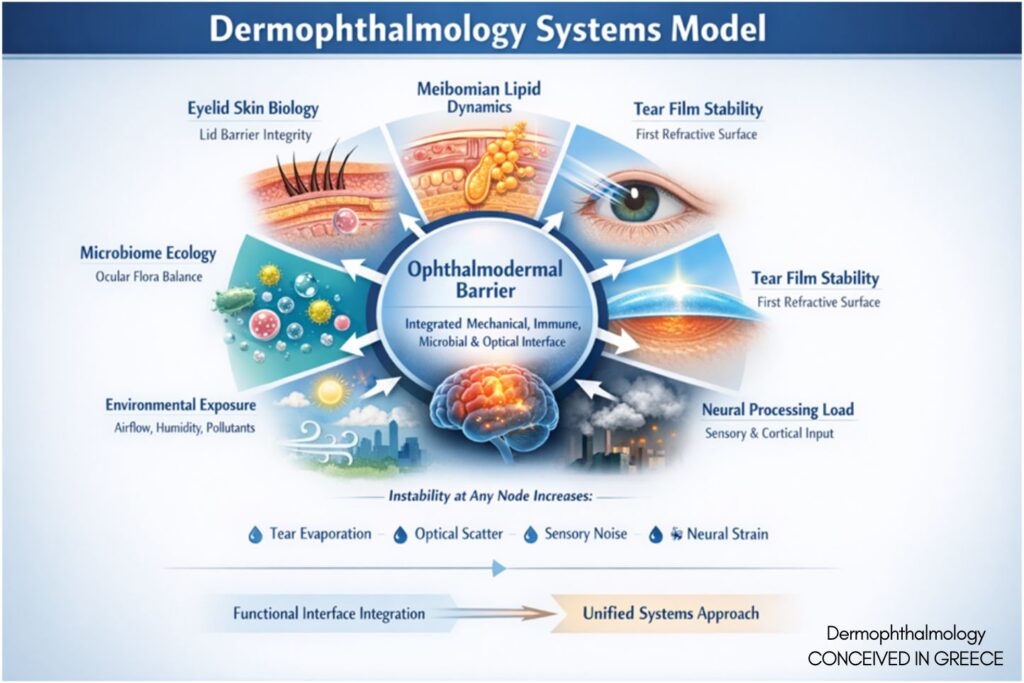
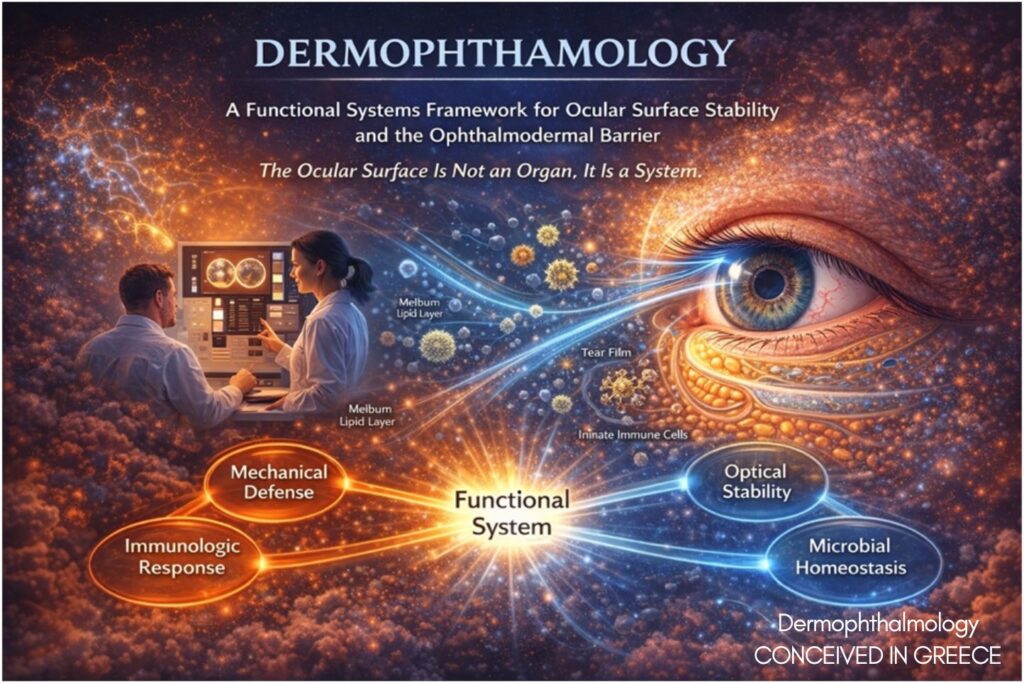
Conceptual Figure Legend
The Dermophthalmology Systems Model
The Dermophthalmology Systems Model illustrates the continuous functional interface between:
1. Skin Biology (Eyelid barrier integrity)
2. Meibomian Lipid Dynamics
3. Tear Film Stability (First refractive surface)
4. Environmental Exposure (Airflow, humidity, pollutants)
5. Microbiome Ecology
6. Neural Processing Load
At the center lies the Ophthalmodermal Barrier, representing the integrated mechanical, immune, microbial, and optical interface.
Instability at any node increases:
• Tear film evaporation
• Optical scatter
• Sensory noise
• Neural compensatory demand
The model emphasizes stabilization of the input layer (ocular surface) rather than isolated symptom suppression.
________________________________________
Conclusion
Tear film dynamics, eyelid biology, microbiome ecology, airflow exposure, and neural processing are not independent variables. They are expressions of a unified biological system. Dermophthalmology does not introduce new biology. It introduces systemic coherence.
________________________________________
References
1. Bron AJ et al. TFOS International Workshop on Meibomian Gland Dysfunction.
2. Nichols KK et al. TFOS DEWS II Definition and Classification Report. Ocul Surf. 2017.
3. Craig JP et al. TFOS DEWS II Environmental Report.
4. Knop E et al. Meibomian glands. Prog Retin Eye Res.
5. Barabino S, Dana MR. Ocular surface inflammation.
6. Tsubota K. Functional visual acuity and dry eye.
7. Goadsby PJ et al. Migraine and central sensitization.
8. Bielory L. Ocular allergy.
9. Kennedy DW. Chronic rhinosinusitis.
10. Barnes PJ. Systemic inflammation in airway disease.
________________________________________
Disclosure Statement
John Tsakalos is conceptually involved in the development of dermophthalmologic translational protocols. The scientific framework presented herein is independent of product-specific evaluation.
