A Dermophthalmologic Approach to Tear Film Stability
Introduction
Why is there so much confusion around artificial tears?
Artificial tears are among the most commonly used eye care products worldwide. Millions of people use them for:
- stinging/burning
- a gritty “sand in the eye” sensation
- redness
- blurry vision
- screen-related eye fatigue
- dry eye
And yet, despite their massive use, most people:
- use them only when discomfort becomes intense
- stop as soon as the symptom improves
- believe they “treat” the problem
- or use them excessively without seeing lasting results
The question is simple:Are artificial tears a treatment?Or are they temporary support?
Dermophthalmology answers clearly:They are not a solution to the system.They are a support tool for the surface.This is not a “detail.” It is a mindset shift.
Because when someone relies on artificial tears as the main solution, it’s like trying to “save” an entire biological structure with a liquid substitute. And the eye does not work that way.
The ocular surface is a system.And every system, to become stable, needs:
- proper function of structures (eyelids – glands)
- a proper “surface” (the tear film)
- proper defense (barrier – microbiome – immune regulation)
- the right environment (humidity – airflow – screens)
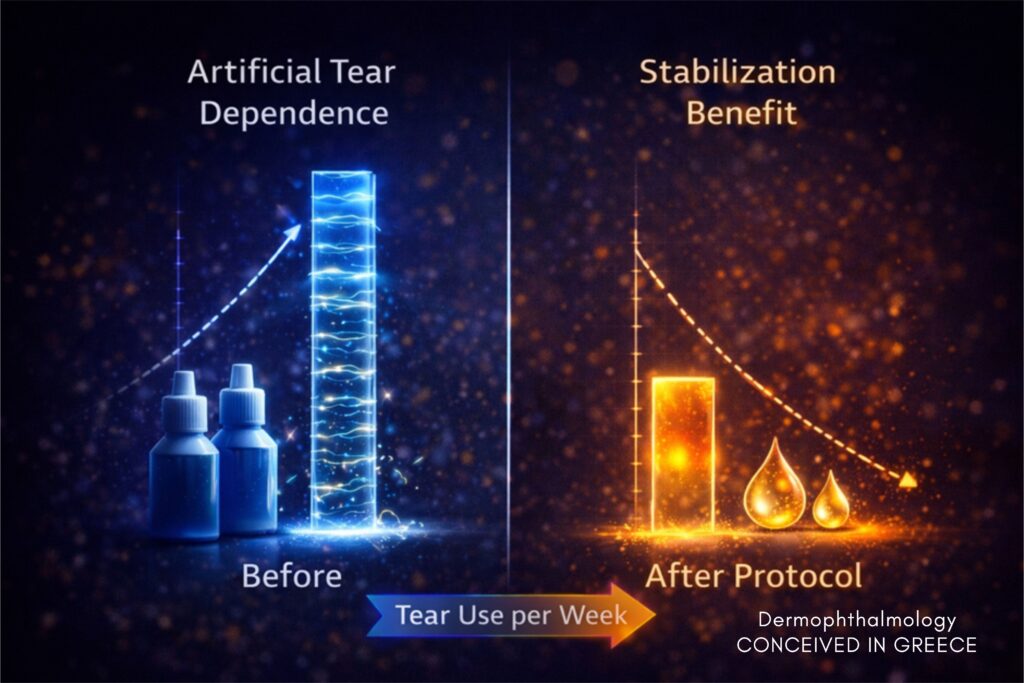
Artificial tears matter. But they are not step one. And when they are placed in the wrong position, they create a vicious cycle: relief → stop → relapse → more use.
And here is the critical point:if you stabilize the eyelid/gland/lipid system, artificial tears “work” far better and last much longer.That is the practical benefit the user must understand.
What is the tear film, really?
The tear film is not simply “water.”It is a dynamic biological system renewed with every blink.It is the surface on which vision “rests.”When it is stable, you see clearly and comfortably.When it is unstable, the eye struggles.
Where does it come from?
The main lacrimal glands, produce the aqueous phase.
Accessory lacrimal glands, contribute to baseline secretion.
Meibomian glands (in the eyelids) produce lipids that form the outer lipid layer.
Conjunctival goblet cells produce mucins that allow proper adhesion/spreading.
The 3 functional layers
Lipid layer
- Reduces evaporation
- Stabilizes the optical surface
- Regulates light scatter
If this layer is weak, the eye loses its “seal.”Then water evaporates quickly—no matter how many artificial tears you instill.
Aqueous layer
- Hydration
- Oxygenation
- Antimicrobial defense
This is where the basic sense of “moisture” belongs. But it is not enough on its own if the lipid layer is compromised.
Mucin layer
- Ensures even distribution
- Stabilizes coherence/adhesion
If the “adhesion substrate” fails, tears do not spread evenly—the film breaks irregularly.
The most important point:
The tear film is the first refractive surface of our optical system(Bron et al., TFOS; Nichols et al., TFOS DEWS II).
It is not only about comfort.It is about visual quality.
Instability means:
- microfluctuations in clarity
- increased light scatter
- reduced contrast
- neural compensatory fatigue, which for many presents as headache or intense visual fatigue
- blurry vision
Stability does not mean simple hydration.It means functional coherence.
What do artificial tears do?
Artificial tears:
- increase aqueous volume
- reduce friction
- temporarily improve clarity
- function as lubricants
They are an:Optical Support Tool.
In simple terms: they give you “time” and “relief” when the system is stressed.
Useful for:
- digital work (reduced blinking)
- dry environments
- air conditioning
- air travel
- postoperative periods
- allergies
- contact lens wear
Especially on screens, many people don’t realize the issue is not just “dryness”: blinking decreases, the film is not spread properly, and lipids are not released effectively.
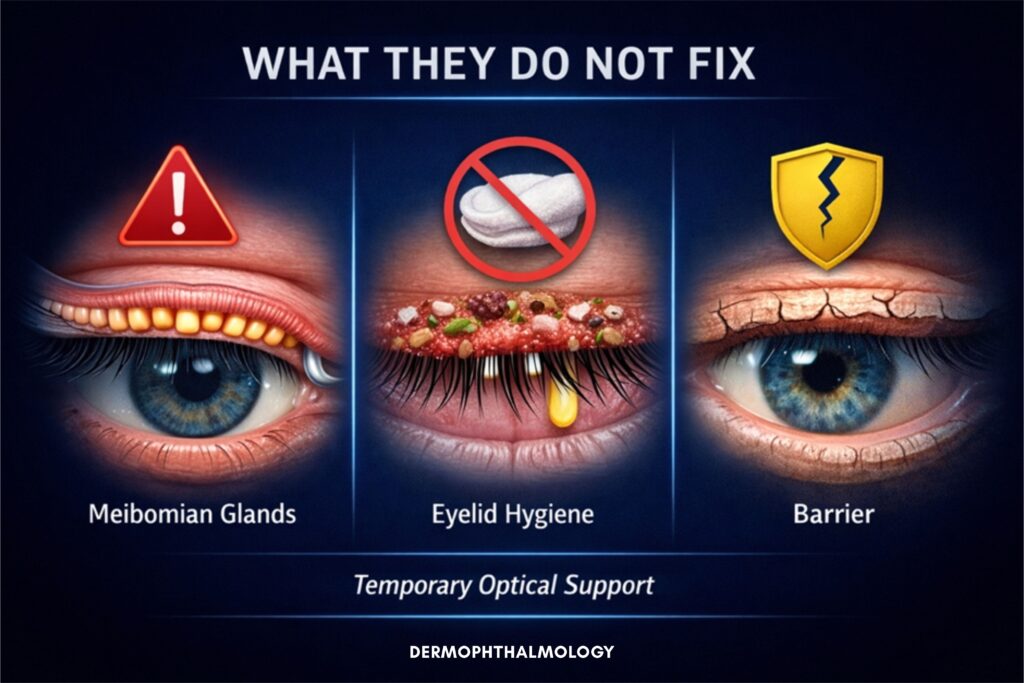
What do artificial tears NOT do?
- They do not open the Meibomian glands
- They do not restore lipid dysfunction
- They do not clean the eyelids
- They do not reduce Demodex
- They do not improve the quality and healthy curvature of eyelashes
- They do not restore the Ophthalmo-Dermal Barrier
If the lipid layer is unstable, their effect is temporary.And that explains why someone may instill artificial tears 3–6 times per day and say:“they help… but soon I’m back to the same.”
It’s not your fault.It’s because you’re using a support tool as if it were a stabilization tool.

The big misconception
Occasional use is like:
- Using mouthwash without brushing your teeth.
- Applying moisturizer without cleansing your face.
- Using hair serum without washing the scalp.
Does it relieve? Yes.Does it fix the system? No.The eye is not just a wet surface. It is a biological system.
And here’s the key:With teeth/skin/hair, everyone understands: first you cleanse and restore, then you support.With eyes, people have learned the reverse: first “drops,” and only later—if ever—attention to the eyelids.
Categories of artificial tears
On the market you may find:
- Sodium hyaluronate + vitamins(e.g., Visionlux Plus Duo, Navitae Plus)
- Sodium Hyaluronate + trehalose(e.g., THEALOZ Duo, THEALOZ Duo Gel)
- Lubricating polymers(e.g., Tears Naturale, Refresh, Vidilac)
- Lipid-enhanced formulations(e.g., Systane Balance / Complete, Artelac)
All primarily aim at:
- hydration
- lubrication
- or lipid support
None, by itself, restores eyelid function.
A practical criterion for users
If you use artificial tears and:
- they last only 5–15 minutes, or
- you need very frequent re-instillation, or
- you feel “something is missing” (as if comfort won’t “lock in”)
then the core issue is very likely functional: eyelids – lipids – barrier, not simple hydration.
Where Dermophthalmology comes in
Dermophthalmology, as promoted by the WOD – World Organization of Dermophthalmology, views the eye as a system.
Tear film stability depends on:
- eyelids
- Meibomian glands
- microbiome
- inflammatory load
- environment
- neuro-sensory processing
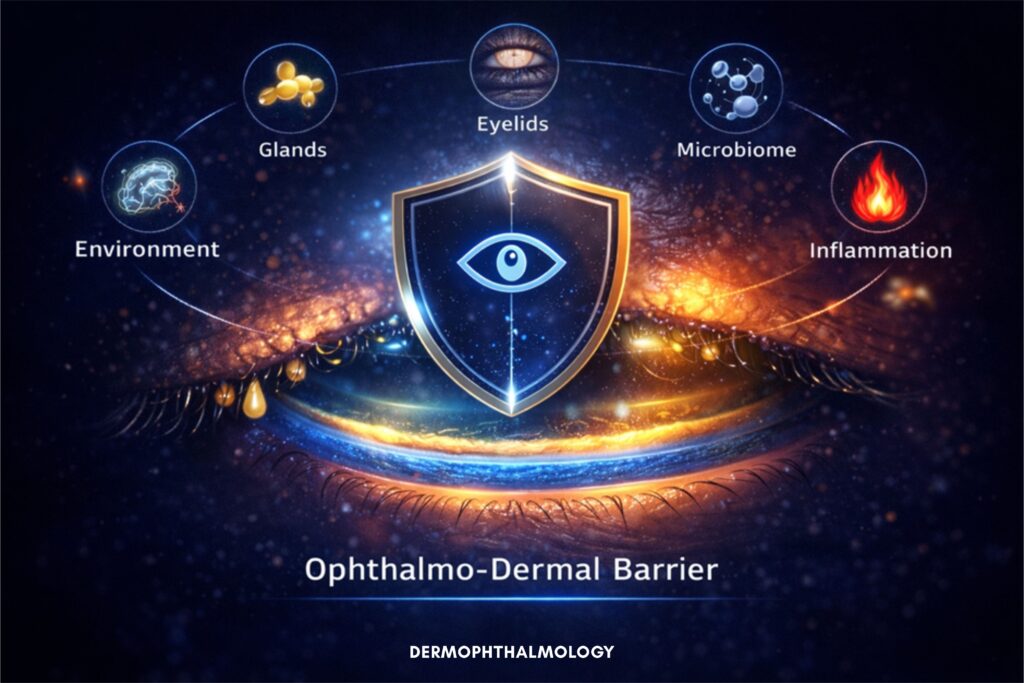
Here we introduce the:Ophthalmo-Dermal Barrier
It includes:
- mechanical protection (blinking)
- lipid stability
- immune regulation
- microbial balance
- the optical surface
When the barrier is unstable:
Artificial tears cover the symptom.They do not restore the system.This is where the Dermophthalmologic logic “locks in”:we don’t chase “more tears.” We chase stability.
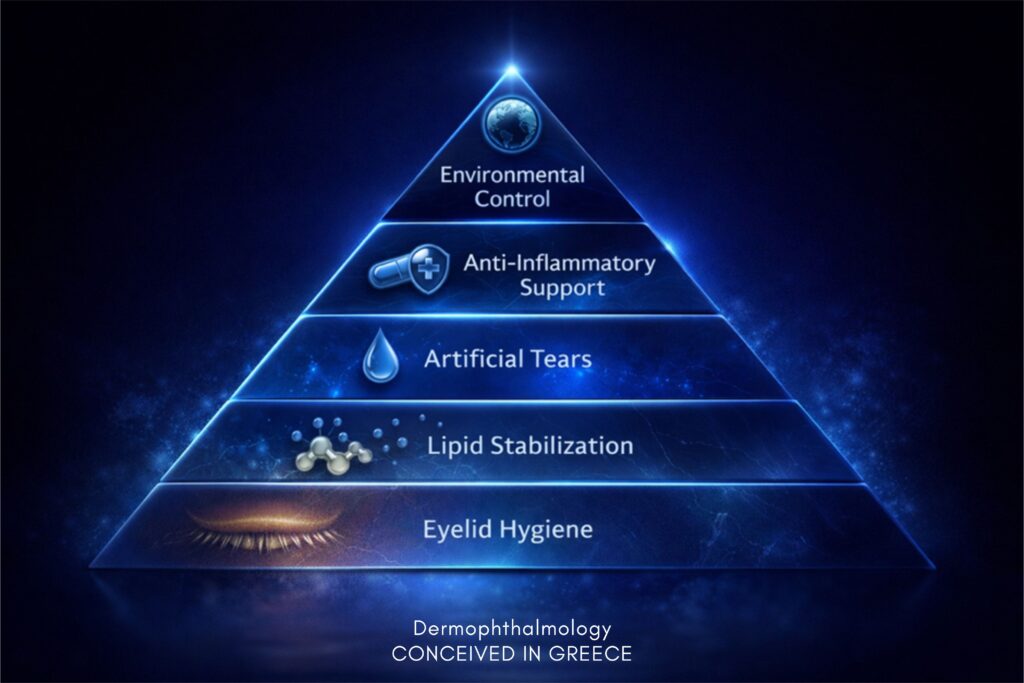
The Dermophthalmologic hierarchy
- Daily eyelid hygiene
- Stabilization of lipid production
- Targeted use of artificial tears
- Anti-inflammatory support
- Environmental control
Artificial tears belong in Step 3—not Step 1.
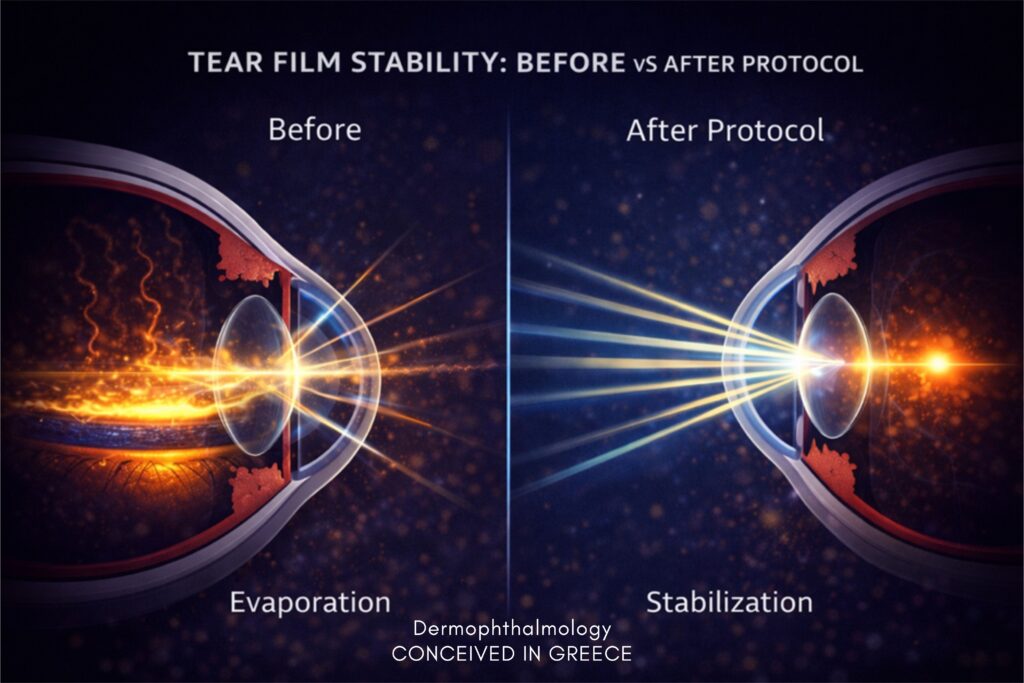
Why is this order “scientifically logical”?
Because the tear film is not only aqueous.If the lipid layer fails, water evaporates.So you begin where the system “seals”: eyelids and glands.
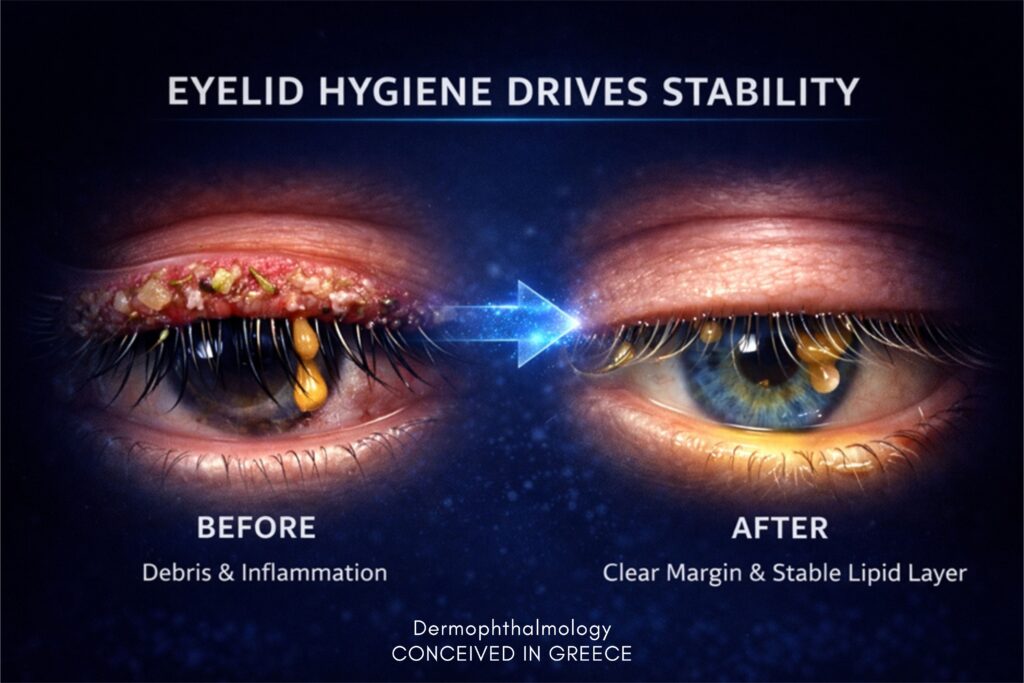
The role of eyelid hygiene
Eyelid hygiene:
- reduces bacterial load
- limits Demodex
- reduces inflammation
- improves lipid flow
- improves eyelash texture
- stabilizes the lipid layer
- improves clarity and quality of vision
When Meibomian glands function properly,artificial tears work better and last longer.
The logic is clear:First you stabilize the system.Then you support it.
How the Ophthalmogen 3-Step Protocol maximizes the benefit of artificial tears
EYE10 → GEL → SPRAY
Here is the practical “game changer” for artificial tear users:If the problem is that tears “don’t last,” the goal is not to add more tears.The goal is to rebuild the ground so they can last.
The Ophthalmogen 3-Step Protocol is designed as an Applied Dermophthalmologic Protocol:
a protocol that works on the system (eyelids–glands–lipids–barrier), so artificial tears become truly effective and you don’t need them “every little while.”
Step 1: Ophthalmogen EYE10 (Thermal Therapy)
What it does to the system:
- applies targeted warmth to the eyelid area
- helps liquefy and improve lipid flow
- supports decongestion of Meibomian glands
- prepares the eyelid to release better-quality oil
What the artificial tear user gains:
- as the lipid layer improves, evaporation decreases
- so tears (natural and artificial) remain longer on the surface
- often fewer instillations are needed during the day
- vision becomes more stable
In other words: EYE10 does not “replace” artificial tears.It makes artificial tears stop being your only defense.
Step 2: Ophthalmogen GEL (Hygiene + Massage + Micro-environment targeting)
What it does to the system:
- supports daily hygiene along the lid margin
- helps reduce microbial/inflammatory load
- supports management of destabilizing factors (e.g., Demodex, subclinical inflammation)
- with gentle massage after EYE10, helps guide the liquefied secretion toward the gland openings
What the artificial tear user gains:
- less inflammation/irritation = less “burning” that triggers drop-seeking
- better eyelid function = better tear film spreading
- over time, the eye is no longer in constant “alarm mode”
- less reflex tearing
Step 3: Ophthalmogen SPRAY (Targeted daily support & stabilization)
What it does to the system:
- provides practical support in environments that “kill” the tear film: screens, A/C, commuting, airplanes
- acts as “external support” for daily stability, especially when blinking is reduced
What the artificial tear user gains:
- reduced need for “drops every little while”
- easier relief without constantly chasing symptoms
- ideal for those who say: “in the office with A/C I’m terrible”
The essence (in one sentence)
Artificial tears support aqueous comfort.
The Ophthalmogen 3-Step Protocol builds the stability conditions so that support can last.In simple terms: the protocol improves the “substrate” (eyelids–lipids–barrier).So drops stop being “rescue” and become what they should be: targeted reinforcement.
Practical application: “How do I combine them during the day?”
For the user who uses artificial tears 3–6 times/day
Goal: gradually reduce instillations—not by “cutting,” but by stabilizing.
Morning or evening (baseline stabilization):
- EYE10 (15–20 minutes, depending on need)
- Gentle eyelid massage with Ophthalmogen Gel (30 seconds)
During the day (where the film “breaks”):
- SPRAY during screens/A/C/dry environments for daily support/stabilization
- Artificial tears targeted only when truly needed (not as the “only weapon”)
Gain:
- longer-lasting relief
- better optical stability
- less symptom-driven “dependence” on drops
Overuse — is there a problem?
Preservatives with chronic use can burden the ocular surface (TFOS DEWS II, 2017).
Continuous use without addressing the cause:
- maintains symptom dependence
- does not solve lipid dysfunction
- does not restore the barrier
It’s not about addiction. It’s about the root cause.
When to suspect something isn’t right
If you need artificial tears:
- every 1–2 hours, or
- daily for months without clear improvement, or
- symptoms feel “odd” (blurs then clears, screen fatigue, burning in A/C)
then a reframe is needed: it’s not only lack of moisture. It’s lack of stability.

When should artificial tears be used correctly?
- during digital work
- in dry environments
- in allergy seasons
- in mild MGD as support
- with contact lenses
- post-operatively
Always as part of a complete care system.
A brief “logic guide”:
- before difficult conditions (flight, screens, A/C) → proactively
- during → targeted (not “panic-driven”)
- after → if needed, but alongside eyelid restoration
Conclusion
Artificial tears:are not a system treatment.They are surface support.Stability comes before discomfort.Prevention comes before relief.
Dermophthalmology repositions them:Not as a solution,but as part of a hierarchy of stabilization.
And when you want to maximize the result (so that relief “lasts”), the logic is:First stabilize the eyelid/lipid/barrier system (EYE10–GEL–SPRAY).Then artificial tears function as what they truly are: targeted support.

FAQ
Can I use artificial tears every day?
Yes—especially preservative-free on the ocular surface such as Visionlux Plus, Navitae Plus, etc. But ideally within a complete care plan.
Do they replace eyelid hygiene?
No. Just as facial moisturizing does not replace facial cleansing, eye “hydration” does not replace eyelid care.
Do they cause addiction?
No. The cause creates the need.
Are they enough for blepharitis?
Usually not.
Correct order?
Hygiene → Lipids → Artificial tears.
If I follow the Ophthalmogen 3-Step, will I stop artificial tears?
The goal is not to “stop” them. The goal is not to depend on them to function. Many people reduce frequency because the system stabilizes.
When does it make sense to use artificial tears if I follow the protocol?
When you have “load” (screens, A/C, travel, contact lenses, allergy) or when you want extra optical comfort. That’s when they work more effectively.
References
- Nichols KK et al. TFOS DEWS II. Ocul Surf. 2017.
- Bron AJ et al. TFOS MGD Report.
- Craig JP et al. TFOS Environmental Report.
- Knop E et al. Prog Retin Eye Res.
- Tsubota K. Functional visual acuity.